Clinical Screening for OSA
TO BE COMPLETED BY A MEMBER OF THE PROFESSIONAL TEAM DURING AN OFFICE VISIT
Has the Patient been Diagnosed with OSA?
Is the Patient being Treated for OSA?
Is the Patient Compliant with Treatment for OSA?
Does the patient have any of the following (check all that apply):
Snoring
Daytime Tiredness/ Drowsiness/ Sleepiness
Observed Pauses in Breathing During Sleep
Age (> 50 Years)
Gender (Male)
Obesity (BMI>30)
Large Neck Size (Men >17” or Women >16”)
GERD (Acid Refulx)
Diabetes
Enlarged Tongue
Narrow Mandible, Retruded Mandible
High Blood Pressure
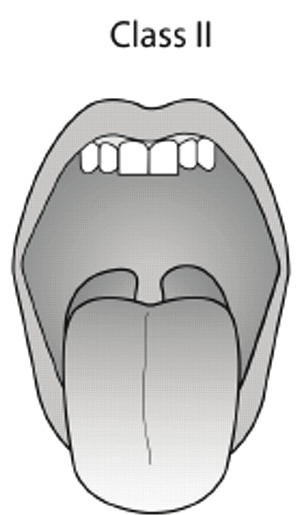
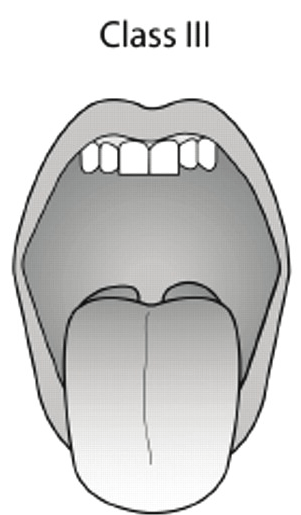
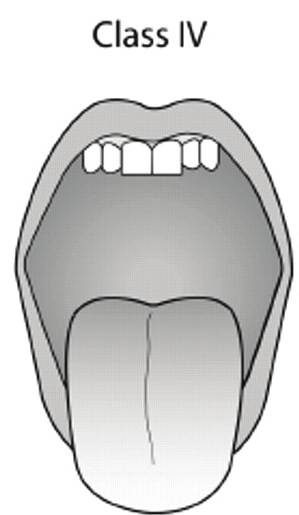
What does the patient’s airway look like (select one)?

Your Score:
CLICK HERE TO KNOW MORE
* >4 number of positive answers and/or a class III or IV airway make it more likely that the patient has obstructive sleep apnea.
© Copyright APP-NEA | All Rights Reserved